 Skip to content
Skip to content
Radiomics
Quantitative imaging biomarkers, AI-driven feature analysis, and the science of reading disease from medical images - CT, MRI, PET, and beyond.
What Is Radiomics?
Radiomics is the discipline of extracting large numbers of quantitative features from medical images - systematically, reproducibly, and at high throughput - to construct imaging biomarkers that can characterize disease biology, inform prognosis, and predict treatment response. Where a radiologist perceives shape, density, and texture qualitatively, radiomics encodes those perceptions as hundreds or thousands of mathematically defined measurements that can be correlated with clinical outcomes and molecular phenotypes.
The term was popularized in oncology research in the early 2010s, but the underlying idea - that medical images contain more quantitative information than is extractable by the human eye - has driven computational imaging research for decades. Scientific output in the field has grown from roughly 120 publications in 2017 to over 1,500 per year by 2023, with the majority concentrated in radiology, oncology, and nuclear medicine.
The central premise of radiomics rests on the principle that imaging phenotypes reflect the underlying biology of tissue: vascularization, cellularity, necrosis, hypoxia, and genetic mutation status can leave detectable signatures in the spatial intensity patterns of CT, MRI, or PET images. Extracting and modelling these signatures at scale - and validating them across independent cohorts - is the core scientific challenge of the field.
Radiomics enables the non-invasive, comprehensive characterization of the entire tumor volume - capturing spatial heterogeneity that a targeted biopsy cannot.
A key advantage of radiomic analysis over tissue biopsy is its non-invasive, whole-tumor coverage. A biopsy samples a small, often peripherally accessible fragment of a tumor. Radiomics, by contrast, can quantify the spatial heterogeneity of the entire lesion volume across every imaging voxel - capturing the intra-tumoral variation that drives drug resistance, recurrence risk, and phenotypic plasticity.
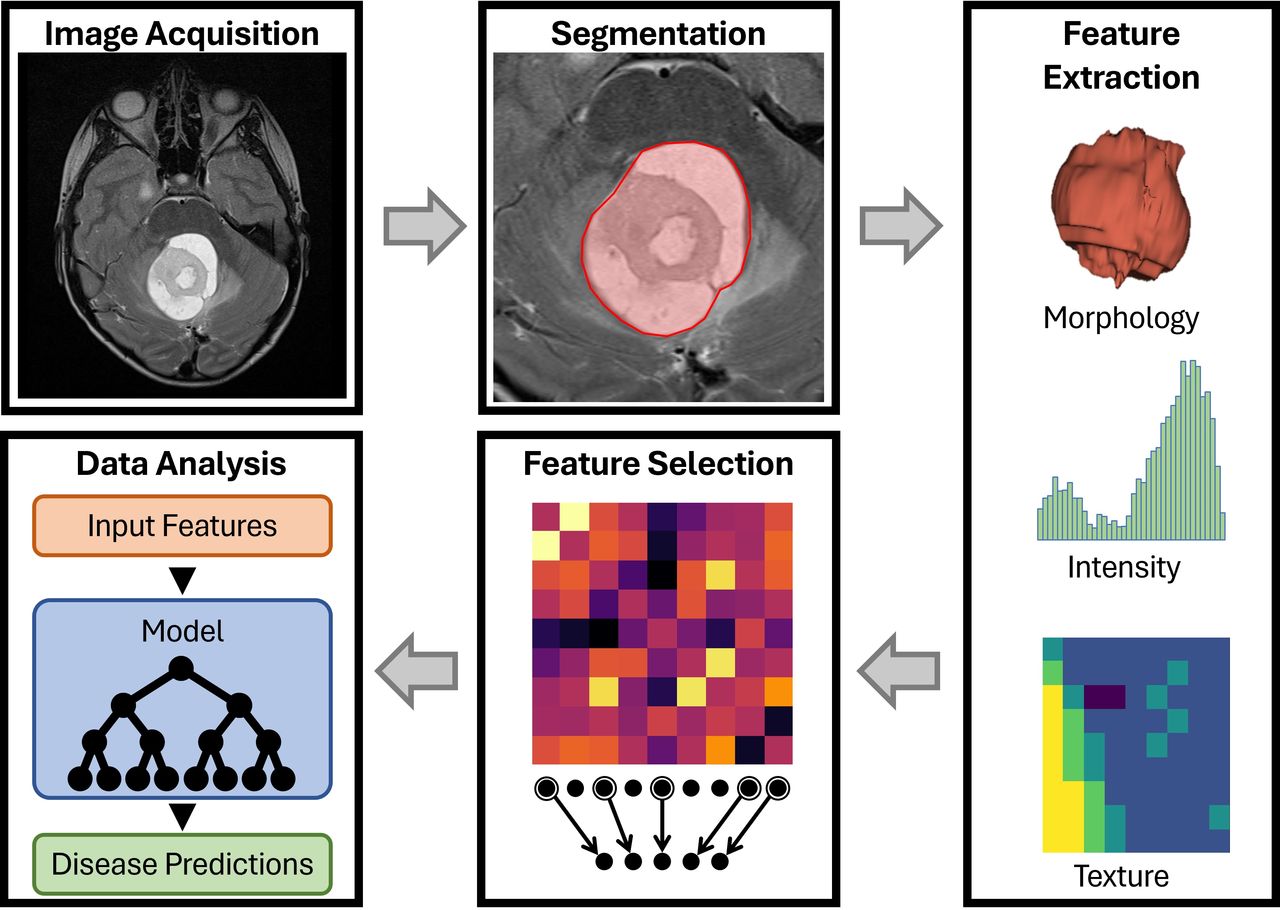
The Radiomics Workflow
A complete radiomics study follows a reproducible, multi-stage pipeline. Each stage introduces potential sources of variability, which is why methodological rigour and standardization at every step are non-negotiable for clinically meaningful findings.
Image Acquisition & Preprocessing
Radiomic features are sensitive to acquisition parameters: CT reconstruction kernel, slice thickness, pixel spacing, MRI echo time and repetition time, PET scanner model, and contrast administration protocol all influence the distribution of voxel intensities. Before feature extraction, raw images must be preprocessed. This typically includes:
- Resampling: Interpolating all images to a consistent voxel size (commonly 1×1×1 mm³) to ensure geometric comparability across scanners and institutions.
- Intensity normalization: Standardizing grey-level ranges, particularly for MRI where absolute signal values are scanner-dependent. Z-score normalization or histogram matching are common strategies.
- Discretization: Binning continuous voxel intensities into a fixed number of grey levels (fixed bin number, FBN) or fixed bin width (FBW) before texture feature computation.
- Image filtering: Applying transforms such as Laplacian of Gaussian (LoG), wavelet decomposition, or gradient filters to generate derived image types that accentuate different spatial scales of texture.
- Bias field correction: For MRI, correcting spatial inhomogeneity in the radiofrequency field that distorts intensity values across the image volume.
Segmentation
Radiomic features are computed within a defined region of interest (ROI) - most commonly the gross tumour volume (GTV), but increasingly also peritumoral tissue, lymph nodes, or organ-at-risk volumes. Segmentation is the single largest source of variability in classical radiomics pipelines. Manual delineation is subject to intra- and inter-observer disagreement; automated deep learning-based segmentation methods are increasingly adopted to reduce this variability and enable at-scale analysis.
Feature Extraction
After preprocessing and segmentation, quantitative features are computed from the voxel intensities within the ROI. A single preprocessing configuration applied to a single image type can yield hundreds of features; applied across multiple filter types (wavelet subbands, LoG at several σ values, square, square root, logarithm, exponential), the feature space routinely reaches 1,000–2,000 dimensions per patient.
Feature Selection & Dimensionality Reduction
Given the high dimensionality of the radiomic feature space relative to typical clinical cohort sizes, aggressive feature selection is essential to avoid overfitting. Common strategies include:
- Reproducibility filtering using the intraclass correlation coefficient (ICC) to retain only features stable across segmentation variations or test-retest scans.
- Univariate correlation filters to remove near-zero variance and highly intercorrelated features.
- Regularized regression (Lasso, Elastic Net) for simultaneous selection and coefficient shrinkage.
- Mutual information and tree-based importance scoring for non-linear feature relevance estimation.
- Dimensionality reduction via PCA or UMAP where interpretability of individual features is less critical.
Model Training & Validation
Radiomic signatures - typically a weighted linear combination of selected features, or a machine learning model - are trained on a labelled dataset and evaluated for their predictive or prognostic performance. The Radiomics Quality Score (RQS) and the Image Biomarker Standardization Initiative (IBSI) frameworks provide checklists for methodological completeness and reproducible reporting. External validation on independent cohorts from different institutions remains the gold standard for demonstrating clinical generalizability.
Feature Taxonomy
Radiomic features are conventionally organized into six major classes, each capturing a distinct geometric or statistical property of the ROI:
Shape & Size Features
Descriptors of the three-dimensional morphology of the segmented region: volume, surface area, sphericity, maximum 3D diameter, surface-to-volume ratio, compactness, elongation, and flatness. Shape features are computed solely from the binary mask and are independent of grey-level intensities.
First-Order Statistics
Statistical moments computed directly from the histogram of voxel intensities within the ROI: mean, median, standard deviation, variance, skewness, kurtosis, energy, entropy, uniformity, and percentile-based range features. First-order statistics describe the overall intensity distribution but are insensitive to spatial relationships between voxels.
Grey Level Co-occurrence Matrix (GLCM)
The GLCM encodes the frequency with which pairs of voxels at a given displacement and direction co-occur with specific intensity combinations. Derived features - contrast, correlation, energy, homogeneity, entropy, cluster shade, cluster prominence - capture the second-order spatial intensity relationships within the ROI.
Grey Level Run Length Matrix (GLRLM)
GLRLM features quantify consecutive runs of voxels with the same intensity along a given direction. Short-run emphasis, long-run emphasis, grey level non-uniformity, and run percentage characterize the coarseness and directionality of texture at the run-length scale.
Grey Level Size Zone Matrix (GLSZM)
The GLSZM captures contiguous regions (zones) of similar intensity within the ROI, encoding both the size of zones and the grey levels they represent. Large zone emphasis features are particularly sensitive to coarse, homogeneous texture regions.
Neighbouring Grey Tone Difference Matrix (NGTDM) & Grey Level Dependence Matrix (GLDM)
NGTDM features (coarseness, contrast, busyness, complexity, strength) measure the difference between a voxel's intensity and the average of its neighbours, characterizing local intensity variation. GLDM features capture how many neighbouring voxels are dependent on a central voxel within a defined intensity window, encoding fine-grained local texture dependence.
IBSI & Standardization
The Image Biomarker Standardization Initiative (IBSI) is the authoritative international framework for defining radiomic feature computation in a mathematically unambiguous way. Established to address the widespread inter-software variability that threatened the reproducibility of multi-centre radiomics studies, IBSI provides:
- Precise mathematical definitions for each feature class and each individual feature.
- A digital phantom with known reference feature values against which software implementations can be benchmarked.
- Standardized preprocessing steps including resampling, intensity discretization, and ROI morphological operations.
- A compliance framework that allows radiomics platforms to declare IBSI conformance at the feature level.
IBSI compliance is now embedded in widely used radiomics platforms, including PyRadiomics, LIFEx, and CERR. Compliance substantially reduces inter-software variability in extracted feature values and strengthens the generalizability of predictive models trained on data from multiple institutions and scanner vendors. Regulatory readiness for radiomics-based clinical decision support tools increasingly depends on demonstrable IBSI alignment.
Despite IBSI standardization, residual variability persists across platforms due to differences in how filters are implemented, edge cases are handled, and floating-point computations are rounded. Prospective multi-site studies routinely quantify inter-platform agreement using intraclass correlation coefficients (ICC), and researchers are advised to extract features using a single, fixed software version throughout a study.
Deep Radiomics
Deep radiomics replaces or augments handcrafted IBSI features with representations learned directly from image data by convolutional neural networks (CNNs), vision transformers (ViTs), or hybrid architectures. The resulting features are sometimes called deep features or deep radiomic signatures.
Several distinct paradigms exist within the deep radiomics landscape:
- Supervised end-to-end learning: A network is trained directly on the clinical endpoint (e.g., survival, treatment response) using image patches or full 3D volumes as input, learning task-relevant representations without manual feature engineering.
- Transfer learning from foundation models: Pre-trained networks (trained on ImageNet, or increasingly on large medical imaging corpora) serve as feature extractors. Their penultimate-layer activations are extracted for the ROI and fed into downstream classifiers, combining the representational power of large-scale pretraining with small medical imaging cohorts.
- Hybrid handcrafted + deep feature fusion: IBSI features and deep features are concatenated or combined via attention mechanisms, exploiting the interpretability of classical radiomics and the representation power of deep networks simultaneously.
- Self-supervised and contrastive pre-training: Models are pre-trained on unlabelled medical images using self-supervised objectives (masked image modelling, contrastive learning), then fine-tuned on labelled radiomics tasks - a promising direction for data-scarce clinical settings.
A persistent tension in deep radiomics is interpretability. Classical IBSI features carry explicit mathematical definitions that clinicians can reason about; deep features are high-dimensional and opaque. Explainability methods - Grad-CAM, SHAP applied to feature vectors, attention weight visualization - are increasingly incorporated to satisfy clinical and regulatory demands for transparency.
Delta-Radiomics
Delta-radiomics - also called longitudinal radiomics - extends the framework from a single imaging time point to the quantification of feature changes across serial scans acquired before, during, or after treatment. The "delta" refers to the signed or absolute difference in a radiomic feature value between two time points, which serves as a dynamic biomarker of treatment-induced biological change.
The clinical motivation is compelling: a tumour that appears visually stable on imaging at the midpoint of chemotherapy may nonetheless show substantial changes in texture, entropy, or heterogeneity features that predict ultimate pathological response. Delta-radiomics can detect these subclinical changes earlier and with greater sensitivity than conventional response criteria such as RECIST.
Key methodological requirements for delta-radiomics include: consistent image acquisition protocols across time points, deformable image registration to align serial scans to a common reference frame, and consistent segmentation propagation. Feature stability across test-retest scans (repeat imaging within days, without clinical change) must be established before longitudinal changes can be interpreted as biologically meaningful.
Habitat Imaging
Habitat imaging partitions the tumour volume into spatially distinct sub-regions - or "habitats" - based on local radiomic feature profiles. Rather than characterizing the tumour with a single radiomic signature averaged across the entire GTV, habitat analysis applies unsupervised clustering (most commonly k-means on voxel-level feature vectors) to reveal the intra-tumoral spatial heterogeneity that a single global signature cannot capture.
Each identified habitat corresponds to a biologically interpretable microenvironmental niche: a hypoxic core, a proliferative rim, a necrotic centre, or an infiltrative margin. These habitats can be annotated with complementary imaging modalities - for example, pairing CT texture habitats with DCE-MRI perfusion or DW-MRI diffusion maps - to link imaging phenotype to underlying tissue physiology.
Habitat imaging is particularly active in hepatocellular carcinoma, clear cell renal cell carcinoma, high-grade glioma, and colorectal liver metastasis research. Three-dimensional habitat features have demonstrated reproducibility and prognostic power advantages over two-dimensional counterparts in several comparative studies.
Multimodal & Multi-Omics Integration
The predictive ceiling of single-modality radiomics is increasingly approached through integration with complementary data domains. Several integration strategies have emerged as productive research directions:
Multimodal Imaging Fusion
Features extracted from different imaging modalities - CT, MRI sequences (T1, T2, DWI, DCE), and PET tracers (¹⁸F-FDG, ⁶⁸Ga-PSMA) - capture complementary aspects of tumour biology. Fusing radiomic signatures across modalities, either by concatenation, attention-based fusion, or ensemble methods, consistently outperforms single-modality models on tasks including survival prediction, grade classification, and treatment response prediction.
Radiogenomics
Radiogenomics correlates imaging phenotypes with genomic or transcriptomic data to non-invasively infer molecular characteristics from images. Established examples include predicting IDH mutation and 1p/19q co-deletion status in glioma from MRI, EGFR mutation probability in NSCLC from CT, and CD8+ tumour-infiltrating lymphocyte density from PET/CT features - enabling virtual "liquid biopsies" from imaging data alone.
Pathomics & Multi-Scale Fusion
Pathomics applies the same quantitative feature extraction philosophy to digitized whole-slide histopathology images. Integrating radiomic (macro-scale morphology) and pathomic (micro-scale tissue architecture) features across spatial scales provides richer tumour characterization than either modality alone.
Clinical & Molecular Data Fusion
Radiomics models routinely benefit from the inclusion of clinical covariates - age, performance status, staging, serum biomarkers - and are increasingly combined with proteomic or metabolomic profiles. Nomogram frameworks and multimodal deep learning architectures are the dominant vehicles for this type of data fusion in the current literature.
Clinical Applications
Radiomics research is most mature in oncology, where the clinical demand for non-invasive, whole-tumour biomarkers is greatest. The following application areas represent the most active and evidenced domains:
Oncology & Cancer Prognosis
Radiomic signatures have been developed for overall survival, progression-free survival, and disease-free survival prediction across virtually every major cancer site - lung, breast, colorectal, liver, head and neck, cervix, prostate, and brain. PET/CT radiomics in diffuse large B-cell lymphoma and NSCLC has been the subject of dedicated international challenges, including the SNMMI AI Task Force Radiomics Challenge.
Treatment Response Prediction
Predicting pathological complete response (pCR) to neoadjuvant chemotherapy or chemoradiation before treatment begins - allowing early escalation or de-escalation - is a high-value application. CT and MRI radiomics models for pCR prediction have been validated in NSCLC, breast cancer, rectal cancer, and soft-tissue sarcoma. Delta-radiomics approaches assessed at early treatment time points further refine these predictions.
Tumour Grading & Molecular Subtype Classification
Non-invasive tumour grading from imaging remains an active target. Clear cell renal cell carcinoma WHO/ISUP grading from CT, glioma IDH status from MRI, and breast cancer molecular subtype classification from DCE-MRI are established research benchmarks. Habitat imaging contributes meaningfully to these tasks by capturing the intra-tumoral heterogeneity that underpins grade.
Immunotherapy Response Biomarkers
With the widespread adoption of immune checkpoint inhibitors, identifying patients who will respond - and distinguishing true progression from pseudoprogression - has become a critical unmet need. PET/CT radiomics has been applied to predict PD-L1 expression and CD8+ tumour-infiltrating lymphocyte density, enabling a non-invasive estimate of the tumour immune microenvironment.
Neuroimaging & Neurological Disease
Radiomics applied to brain MRI extends beyond oncology into neurodegenerative disease characterization, surgical outcome prediction in chronic subdural haematoma, epilepsy focus localization, and white matter lesion quantification. Structural and functional neuroimaging radiomics is an emerging interface between classical MRI analysis and machine learning.
Challenges & Open Problems
Despite the volume of published radiomics research, the field faces substantial methodological and translational challenges that limit clinical adoption. Understanding these challenges is essential for producing rigorous, reproducible radiomics research.
Reproducibility & Harmonization
Feature values are sensitive to acquisition protocol, scanner vendor, reconstruction kernel, and voxel size. Multi-site studies routinely observe that scanner-induced variability can rival or exceed the biological signal of interest. Harmonization methods - including ComBat statistical harmonization, deep learning-based image harmonization, and federated learning across institutional sites - are active research responses to this problem.
Small Cohort Sizes & Overfitting
Many published radiomics studies train models on cohorts of 50–200 patients against feature spaces of hundreds to thousands of dimensions - a combination virtually guaranteed to produce optimistic internal performance estimates that fail to replicate externally. Proper nested cross-validation, stratified splits, and mandatory external validation on independent cohorts are methodological requirements that the field is increasingly enforcing through reporting guidelines (METRICS, TRIPOD+AI, RQS 2.0).
Segmentation Variability
Manual tumour delineation introduces intra- and inter-observer variability that propagates into extracted feature values and reduces the effective reproducibility of radiomic signatures. Automated deep learning segmentation improves consistency but requires its own validation across scanner types and imaging conditions.
Interpretability & Clinical Trust
A radiomic signature that achieves high AUC on a validation dataset is clinically actionable only if its mechanism can be understood and trusted by clinicians. The "black box" criticism applies particularly to deep radiomics models. SHAP-based feature attribution, attention visualization, and alignment with known biological mechanisms are important steps toward interpretable radiomic AI.
Regulatory Pathway
Radiomics-based clinical decision support tools face jurisdiction-specific regulatory requirements - FDA 510(k) or De Novo pathways in the United States, CE marking under EU MDR in Europe, and CDSCO oversight in India. Demonstrating analytical validity, clinical validity, and clinical utility across diverse patient populations is the regulatory standard. No radiomics-based tool has yet achieved broad regulatory approval as a standalone diagnostic or prognostic device, though the pipeline is maturing rapidly.
Bias & Fairness
Radiomic models trained predominantly on data from high-income, high-resource imaging environments may not generalize to populations scanned on different equipment or following different clinical protocols. Bias analysis across race, sex, age, and institution is now an emerging requirement for publications targeting clinical translation.
Key Tools & Software
The following open-source tools form the practical foundation of most academic radiomics research. Each is IBSI-compliant or IBSI-aware, and integration into reproducible analysis pipelines is strongly recommended.
- PyRadiomics - The dominant open-source Python library for radiomic feature extraction (van Griethuysen et al., 2017). Implements the full IBSI feature set across all six feature classes, supports original and filter-derived images (LoG, wavelet, square, square root, logarithm, exponential, gradient), and integrates natively with 3D Slicer for interactive analysis.
- LIFEx - A Java-based, IBSI-compliant freeware with an interactive graphical interface for visualization, segmentation, and feature extraction across PET, CT, MRI, and SPECT images. Widely used for multi-site studies.
- CERR (Computational Environment for Radiological Research) - A MATLAB-based platform supporting IBSI-compliant feature extraction alongside treatment planning data, enabling combined dosiomics and radiomics analysis.
- 3D Slicer - An open-source, extensible medical image analysis platform that serves as a graphical front-end for PyRadiomics and hosts the SlicerRadiomics extension for accessible GUI-driven feature extraction.
- SimpleITK / ITK - The foundational image processing libraries underlying most Python-based radiomics pipelines, providing DICOM I/O, resampling, registration, and morphological operations.
- Pyfeats / OpenCV / scikit-image - Supplementary libraries used for two-dimensional texture analysis, shape morphology, and custom filter implementations.
- scikit-learn / lifelines / scikit-survival - Standard machine learning and survival analysis libraries used for model training, cross-validation, and time-to-event outcome modelling in radiomics pipelines.
Articles in This Series
The articles below constitute the Radiomics series on this platform. Each is written to the standard of a technical research note - precise, referenceable, and appropriate for graduate students, clinical researchers, and ML engineers entering the field.